|
Clinical Advances in Hematology & Oncology February 2022 - Volume 20, Issue 2 Evolving Management of Patients With Double-Hit Lymphoma 双重打击淋巴瘤的演变 Ann S. LaCasce, MD, MMSc
Director
Dana-Farber/Mass General Brigham Fellowship in Hematology/Oncology
Fellowship Program in Hematology/Oncology Chair
Associate Professor of Medicine
Harvard Medical School
Boston, Massachusetts
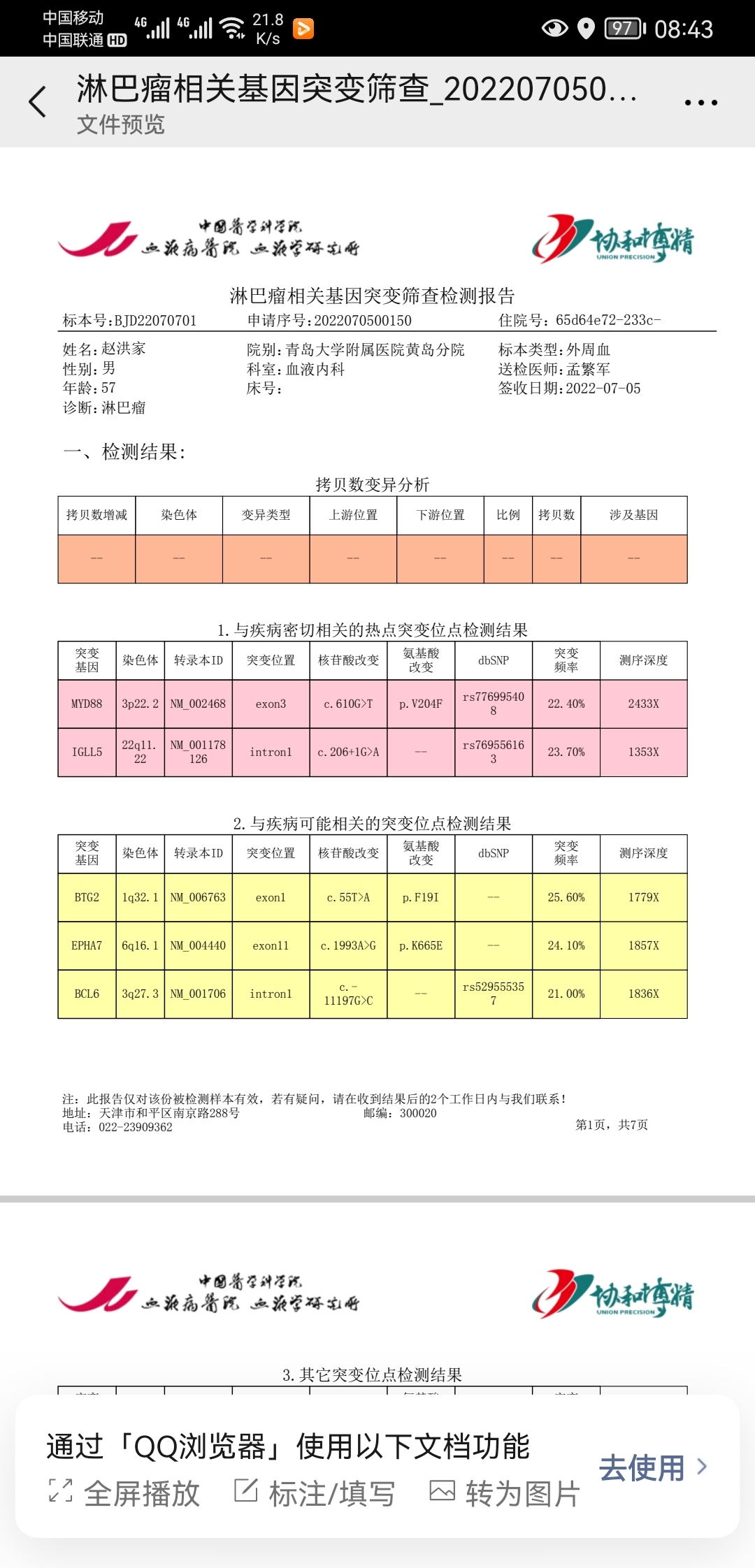
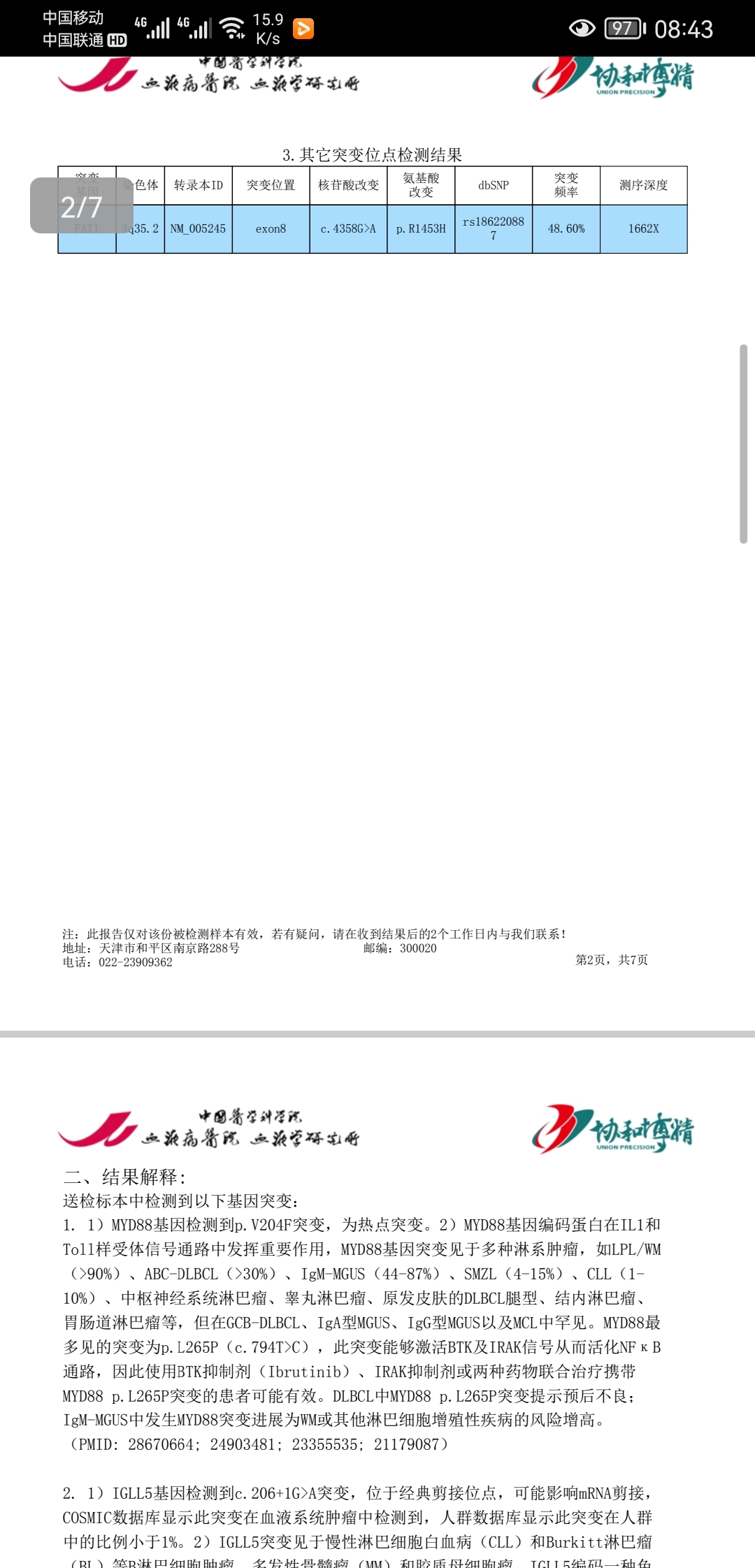
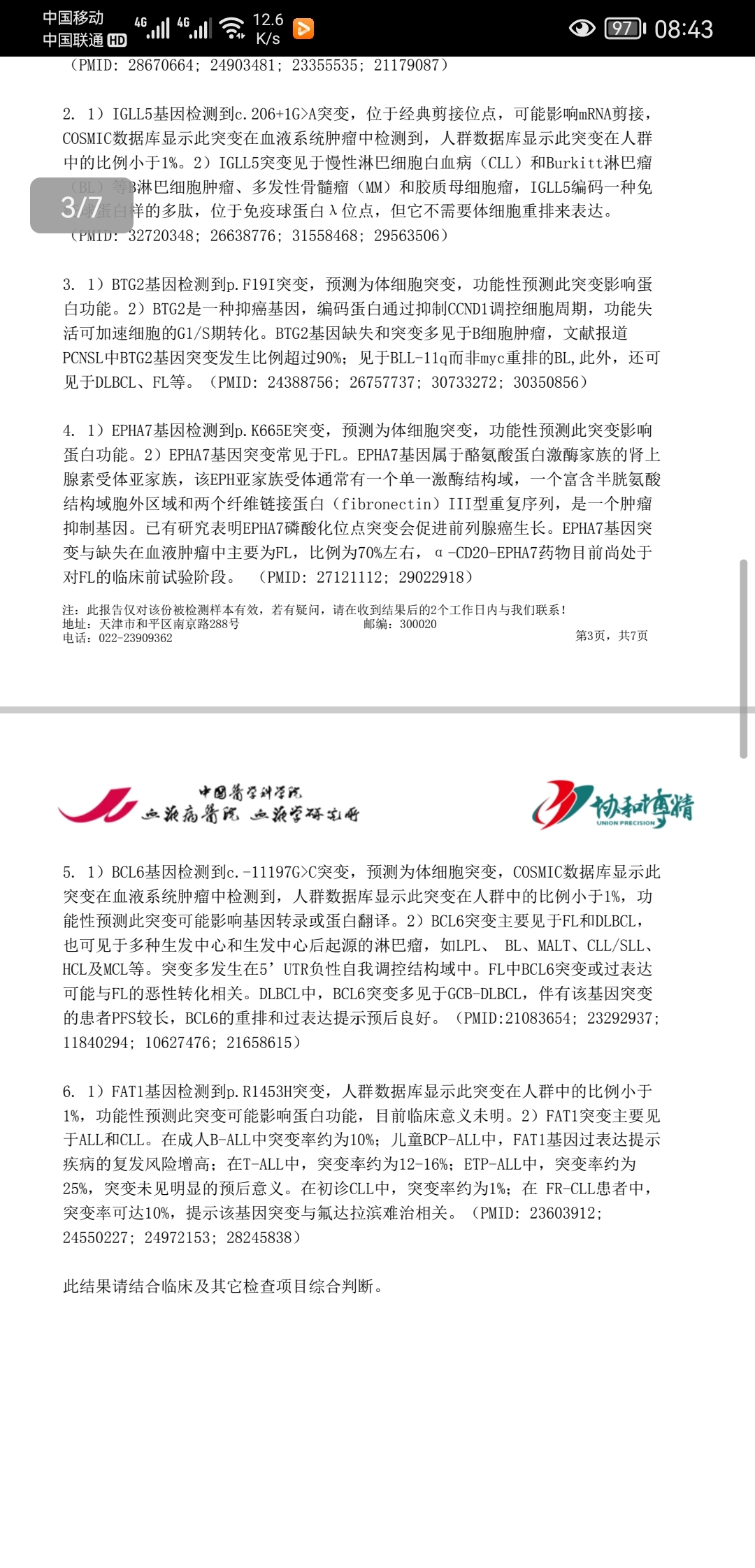
H&O What is the definition of double-hit lymphoma? 双重打击淋巴瘤的定义是什么? AL Double-hit lymphoma is an aggressive B-cell lymphoma with MYC translocation and a BCL2 and/or BCL6 translocation. The diagnosis requires a rearrangement of the genes, rather than extra copies. 双重打击淋巴瘤是一种具有MYC易位和BCL-2或BCL-6易位的侵袭性的B细胞淋巴瘤。确诊需要有基因重排,而不是拷贝数增加。 H&O What are the clinical features of double-hit lymphoma? 双重打击淋巴瘤的临床特点是什么? AL Most patients tend to present with aggressive, symptomatic disease with extranodal sites, a high International Prognostic Index score, and high levels of lactate dehydrogenase. Recently though, we have seen more reports of double-hit lymphoma in patients with lower-stage disease that appears less clinically aggressive. At my institution and many others, pathologists routinely perform fluorescence in situ hybridization (FISH) to check for a MYC rearrangement in all patients with diffuse large B-cell lymphoma (DLBCL) or high-grade B-cell lymphoma. From a pathologic perspective, double-hit lymphoma can appear identical to standard DLBCL. A small subgroup of patients have disease with a more aggressive histologic appearance, similar to Burkitt lymphoma. These patients typically have BCL2 translocations or overexpression. If a pathologist performs a workup for Burkitt lymphoma in these patients, he or she will find that the immunophenotypic characteristics do not support this diagnosis and will therefore perform FISH to evaluate for double-hit or triple-hit lymphoma. 大多数患者呈现为侵袭性、系统性疾病,有结外侵犯,有更高的IPI指数,以及较高的LDH值。不过,最近我们也见到了更多的临床上侵袭性不是很强,分期也较早但却是双重打击淋巴瘤的报道。在我们医院和很多其它一些医院里,病理医生对全部弥漫大B细胞淋巴瘤和高级别B细胞淋巴瘤患者常规性的做FISH检查MYC重排。从病理学角度讲,双重打击淋巴瘤可以看上去与标准的弥漫大B细胞淋巴瘤没有什么两样。有一小部分患者的疾病在组织学上与伯基特淋巴瘤相似,看上去侵袭性很强。如果病理医生对这些患者做伯基特淋巴瘤的免疫组化套餐,会发现在免疫表型上不支持伯基特淋巴瘤的诊断结论,然后会做FISH筛查双重打击或三重打击。 H&O Are there any recent insights into the biology of double-hit lymphoma? 最近对双重打击淋巴瘤有什么新的认识吗? AL Most cases of double-hit lymphoma fall into the germinal center B-cell (GCB) subtype in the cell-of-origin classification. Investigators such as Drs Margaret Shipp and Louis Staudt have moved beyond the cell of origin to identify more refined subgroups of aggressive B-cell lymphoma using comprehensive assessments of gene mutations and copy number changes. Double-hit lymphoma falls into the EZB group in Staudt’s LymphGen classification and cluster 3 in Shipp’s DLBCL clusters. 大多数双重打击淋巴瘤按照细胞来源的分类属于生发中心亚型。一些研究者比如Drs Margaret Shipp和Louis Staudt通过综合分析基因突变和拷贝数改变对侵袭性B细胞淋巴瘤做了更细致的亚组分型。双重打击淋巴瘤在Staudt’s LymphGen分类系统中归纳在EZB组中,在Shipp’s的分组中被归纳在第3组。 Ongoing research is further evaluating additional factors contributing to the poor prognosis of these patients. A large analysis from the Lunenburg Lymphoma Biomarker Consortium found that patients in whom MYC is partnered with an immunoglobulin gene, most commonly the heavy-chain gene, appear to have the most aggressive course and worse outcome compared with other gene partners. Most pathologists assess for MYC rearrangements using a break-apart probe, where the partner gene is not identified. In the future, however, more centers may evaluate for the partner gene, particularly if data confirm that immunoglobulin partner genes drive poor outcomes. 目前的一些研究在进一步的分析造成这些患者不良预后的其它因素。Lunenburg Lymphoma Biomarker Consortium发现,如果MYC重排的伙伴基因是一个免疫球蛋白基因,最常见的是免疫球蛋白重链,似乎侵袭性是最强的,预后也是相对来说最差的。大部分病理医生用分离式探针检查MYC重排,因此无法确定重排的伙伴基因是什么。将来,更多的中心可能会分析伙伴基因,尤其是当有更多数据确认免疫球蛋白伙伴基因会造成不良预后之后。 The prognostic implication of a BCL6 rearrangement is controversial. Recently, there has been some question as to whether patients with MYC and BCL6 rearrangements have the same poor outcomes with standard rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) as patients with double-hit lymphoma with MYC and BCL2 rearrangements. In the study by the Lunenburg Consortium, prognosis appeared to be similar in both groups of patients, although the numbers were small. BCL-6重排的预后意义存在争议。最近,关于MYC和BCL-6重排的患者是否在标准的R-CHOP治疗下与MYC和BCL-2重排的患者有同样的不良预后出现了一些疑问。Lunenburg Consortium所做的研究中,两组患者的预后看起来是相似的,不过样本数量偏少。 H&O How does double-hit lymphoma differ from other lymphomas? 双重打击淋巴瘤与其它淋巴瘤有什么不同? AL Outcomes with R-CHOP are much worse in patients with double-hit lymphoma vs non–double-hit DLBCL. Researchers have studied the use of more aggressive chemotherapy regimens, such as those used in Burkitt lymphoma, including a modified Magrath regimen; fractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (hyper-CVAD); and dose-adjusted rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin (R-EPOCH). 在R-CHOP方案治疗下,双重打击淋巴瘤的结局比非双重打击淋巴瘤要差的多。研究人员尝试了各种更强的方案,比如通常用于伯基特淋巴瘤的方案,包括改良的Magrath方案,HyperCVAD方案,和DA- EPOCH-R方案。 In retrospective series, these treatments appear to improve progression-free survival, but not necessarily overall survival. Only one prospective phase 2 study has examined the treatment of MYC-rearranged aggressive lymphomas. 在回顾性研究中,这些方案看起来是改善了无进展生存,但是并不一定带来了总生存的获益。关于MYC重排的侵袭性淋巴瘤治疗的临床研究中,只有一项二期研究是前瞻性。 This multicenter study, performed by Dr Kieron Dunleavy and colleagues, evaluated treatment with dose-adjusted R-EPOCH. The trial enrolled patients with both single-hit and double-hit lymphomas. At 48 months, the rate of event-free survival among the entire population was 71%. Treatment with R-EPOCH led to better outcomes than expected, which might be attributable to the patient population. Patients with double-hit lymphoma are often too sick to participate in clinical trials. Enrolling patients on studies takes time and can sometimes be difficult in hospitalized populations. When patients need immediate therapy, we will often initiate treatment with R-CHOP. We are aware that these patients may in fact have double-hit lymphoma, and that treatment will need to transition to dose-adjusted R-EPOCH. It is unclear whether the population in the prospective study reflects the typical group of patients we treat with double-hit lymphoma. Double-hit lymphoma can also arise in the context of an underlying follicular lymphoma that transforms after previous treatment. Outcomes are much worse among patients who were previously treated with cytotoxic chemotherapy. 这项Dr Kieron Dunleavy等人主持的多中心研究,评估了DA-EPOCH-R方案。试验纳入了单打击和双重打击的患者。在48个月时,整个患者群体的无事件生存率是71%。R-EPOCH方案治疗的效果比预想的要好,可能与患者群体有关。双重打击淋巴瘤患者经常病的太重以至于无法参加临床试验。患者入组需要很长时间,有时候对于住院患者来说困难很大。当患者急需治疗时,我们一般会先用R-CHOP。我们知道,这些患者中有的实际上是双重打击,需要在后面过渡到DA- EPOCH-R方案。不太清楚这项前瞻性研究的试验人群是否代表了典型的双重打击淋巴瘤。双重打击淋巴瘤有时也会在经过治疗后又发生了转化的滤泡性淋巴瘤患者当中出现。如果患者先前接受过细胞毒的化疗,结局会非常不好。 Some patients with double-hit lymphoma have extensive bone marrow disease, sometimes with lymphoma circulating in the blood. This scenario is particularly challenging to treat, and these patients have a very high risk of central nervous system (CNS) involvement. Intrathecal chemotherapy does not adequately penetrate the brain parenchyma. Administration of systemic methotrexate with dose-adjusted R-EPOCH is difficult. These patients represent an unmet need. 一些双重打击淋巴瘤的患者存在广泛的骨髓侵犯,有时外周血中也有淋巴瘤。这种情况非常难治,而且这类患者有非常高的中枢神经系统侵犯的风险。鞘注不能够有效的穿透脑实质。系统性的甲氨蝶呤与DA-EPOCH-R方案很难联合使用。这些患者属于未能满足的医疗需求。 H&O Does the evaluation process differ for patients with double-hit lymphoma? 双重打击淋巴瘤的检查过程与其它有什么不同吗? AL Clinicians may evaluate the cerebral spinal fluid at baseline in high-risk patients, even in the absence of symptoms. Until recently, most academic centers administered CNS prophylaxis to patients with high-risk DLBCL. Recent data, however, suggest that this strategy is not effective in these patients. The value of CNS prophylaxis in double-hit lymphoma is unclear and controversial. 对于高风险患者,临床医生会在基线检查时分析脑脊液,即使没有中枢神经系统侵犯的相关症状。直到最近,大多数医疗中心对高风险大B患者做CNS预防。不过,最近的数据提示,这个策略对这些患者来说并没有效果。双重打击淋巴瘤的CNS预防的价值,既不明确也充满争议。 H&O What factors guide treatment selection in double-hit lymphoma? 哪些因素指导双重打击淋巴瘤的治疗? AL Currently, patients with double-hit lymphoma receive dose-adjusted R-EPOCH. R-CHOP is not adequate, as outcomes are inferior to those seen in DLBCL. In the prospective study, the rate of event-free survival was 71%. However, the rate in clinical practice is somewhat lower, likely given the selection bias toward enrollment of healthier patients in phase 2 studies. For young patients with double-hit lymphoma, particularly those with extensive disease in the bone marrow, options include the modified Magrath regimen or hyper-CVAD. These treatments include CNS-directed therapies. Pediatricians use these very aggressive regimens in patients with Burkitt lymphoma and DLBCL. Prospective clinical trials are needed. 目前,双重打击淋巴瘤采用DA-EPOCH-R方案。R-CHOP是不适合的,结局会比一般的大B差。在前瞻性的研究中无事件生存率是71%。但是,在临床实践中,生存率没有这么高,大概是因为二期临床研究中收治的患者相对来说要健康一些吧。对于年轻的双重打击患者,特别是有骨髓广泛侵犯的患者,可选方案也包括Magrath方案或HyperCVAD。这些还包括针对CNS的治疗。儿科医生对伯基特或弥漫大B的儿童患者采用非常激进的方案。我们需要更多的前瞻性的临床研究来指导临床实践。 H&O Are there any promising novel treatments? 有没有什么很有希望的新疗法? AL Chimeric antigen receptor (CAR) T-cell therapy provides a glimmer of hope for patients with primary refractory or relapsed disease. Although the reported number of patients is small, outcomes appear to be encouraging in double-hit lymphoma. By targeting CD19 on the lymphoma cell surface, CAR T-cell therapy has a completely different mechanism of action and may be effective in patients whose disease is resistant to standard chemotherapy. CAR T cells may be used earlier in high-risk patients. CAR-T疗法为原发耐药或复发的患者带来了一线希望。尽管报告的病例数还不多,但是对双重打击来说很令人鼓舞。通过靶向于淋巴瘤细胞表面的CD19,CAR-T疗法的作用机制完全不同于以往,对标准治疗耐药的患者可能有效。高风险的患者CAR-T可能要提前使用。 In addition, a number of novel drugs that target cell-surface markers, such as tafasitamab-cxix (Monjuvi, Morphosys/Incyte), loncastuximab tesirine-lpyl (Zynlonta, ADC Therapeutics), and polatuzumab vedotin-piiq (Polivy, Genentech), may be effective in double-hit lymphoma. More data are needed. 此外,一系列靶向于细胞表面标记物的新药,例如CD19单抗,CD19 ADC,以及CD79b ADC等对于双重打击也可能有效。目前还需要更多数据。 H&O What are the unmet needs in double-hit lymphoma? 双重打击的未满足的医疗需求怎么办? AL Traditionally, outcomes in patients with double-hit lymphoma have been poor, particularly for those with concurrent CNS disease. Many patients are resistant to initial therapy and develop rapidly progressive, chemotherapy-refractory disease. Treatment with rituximab, ifosfamide, carboplatin, and etoposide (RICE) or standard salvage regimens is rarely effective, and few patients make it to stem cell transplant. Thankfully, we now have CAR T-cell therapy and other novel approaches. One of the first patients I enrolled on a CAR T-cell trial with double-hit lymphoma remains in a durable remission 5 years after treatment. 传统上说,双重打击淋巴瘤的预后可能不好,特别是并存CNS疾病的患者。很多原发耐药,并进展迅速。挽救性化疗方案,包括RICE等很少奏效,很少的患者能过渡到自体造血干细胞移植。谢天谢地,我们现在有了CAR-T和其它新药。我最早入组CAR-T研究的一位双重打击患者在治疗后到现在为止已经缓解5年了。 Incorporating these novel agents and approaches earlier in the treatment course will likely lead to better responses. When these patients become sick, they are often highly symptomatic and tolerate any therapy poorly owing to their poor performance status and the organ toxicity caused by the disease or cytotoxic chemotherapy. 在治疗过程中较早的引入新药和新的疗法有可能会带来更好的效果。当这些患者病起来的时候,通常症状严重,而且由于疾病本身对器官影响,或者先前化疗的原因以及体能状态不佳对任何疗法的耐受性都很差。 H&O Are there any other areas of research in double-hit lymphoma? 在双重打击淋巴瘤上还有哪些领域在开展研究? AL Scientists are trying to better understand the biology of double-hit lymphoma and disease heterogeneity to identify potential therapeutic targets. In lymphoma, we have amazing laboratory-based scientists who are dedicated to the field. Many advances have already been made, and I am hopeful that management of these patients will continue to improve. 科学家们正在试图更好的了解双重打击淋巴瘤的生物学特性,以及疾病的异质性,以便找到潜在的靶点。在淋巴瘤上,我们有出色的实验室科学家专门致力于这个领域。已经有很多成果,有望进一步改善对患者的管理。 H&O Do you have any other observations regarding the management of patients with double-hit lymphoma? 你对双重打击淋巴瘤的管理是否还有其它的一些见解? AL From a clinical perspective, it is important to recognize patients with aggressive disease early. In the patients with localized disease that is clinically less aggressive, we need studies to determine optimal management. It is not known whether they need more aggressive treatment or if they may do well with R-CHOP. Fewer than 10% of patients with aggressive lymphoma have double-hit lymphoma. It is critical for scientists and clinicians to work together to study this disease from both biologic and therapeutic perspectives. 从临床的角度说,尽早确认疾病的高侵袭性很重要。对于局限期,临床侵袭性不是很强的患者,我们需要通过临床研究确定最佳的治疗方法。还不知道他们是否需要比R-CHOP更强的方案。侵袭性淋巴瘤中不到10%是双重打击淋巴瘤。科学家和临床医生需要通过协作从生物学和诊疗学两个方向来研究这个疾病。 Disclosure Dr LaCasce has no relevant conflicts of interest to report.
| 
 [复制链接]
[复制链接]
 /1
/1 




 窥视卡
窥视卡 雷达卡
雷达卡


 发表于 2022-5-28 16:47:12
发表于 2022-5-28 16:47:12
 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 抢沙发
抢沙发 显身卡
显身卡 发表于 2022-5-28 19:00:37
发表于 2022-5-28 19:00:37

 楼主
楼主